This study explored the developmental potential of MI oocytes that did not respond to rescue IVM. The findings indicate that, despite their well-known limitations compared to in vivo matured MII oocytes, immature MI oocytes can still undergo fertilization, embryo development, and even result in pregnancy. These results highlight the possibility that MI oocytes, which are usually discarded in routine IVF practice, may represent an additional resource for patients undergoing assisted reproduction.
A significant and unresolved issue in IVF-ICSI cycles is immature oocytes. In standard practice, insemination is performed exclusively on MII oocytes. While rates vary slightly between studies, approximately 4% of collected oocytes are in metaphase I (MI) and 11% are at the germinal vesicle (GV) stage [10, 11, 12]. Other studies have reported that around 20% of oocytes are immature [13]. Even though the clinical efficacy and safety of in vitro maturation in stimulated cycles in a subject of ongoing debate, rescue IVM is routinely applied to all MI oocytes, regardless of the patient’s MII oocyte count, as part of a strategy to optimize cycle outcomes in our INF Unit, because each mature oocyte contributes to cumulative pregnancy and live birth rates [14]. Additionally, a higher proportion of immature oocytes within the total yield is associated with reduced pregnancy potential of mature sibling MII oocytes [8]. For this reason, every MI oocyte is considered valuable. If MI oocytes extrude the first polar body within a few hours, they are rescued, matured in vitro, and subsequently inseminated. Approximately 60% of immature oocytes progress to the MII stage [14]. However, when IVM fails and MI oocytes do not mature, they are typically discarded in most IVF units.
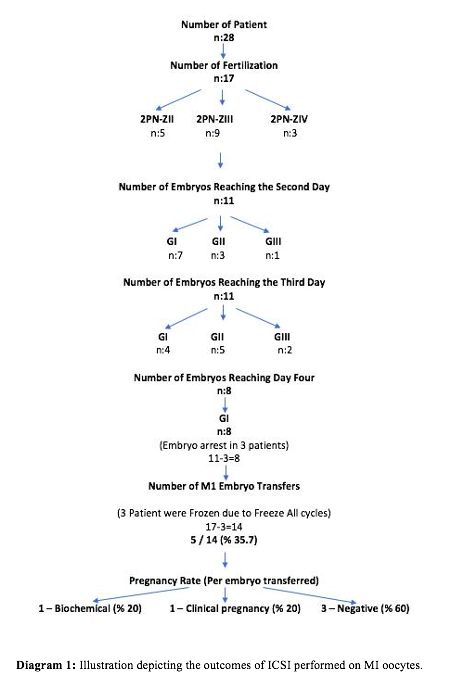
In this study, MI oocytes that failed to mature following rescue IVM demonstrated measurable developmental potential, with clinically relevant fertilization and embryo formation rates. Polarized light microscopy revealed that MI oocytes are not a uniform population. In a subset of MI oocytes, a well-defined metaphase spindle was observed despite the absence of the first polar body, suggesting that these oocytes had initiated nuclear maturation and may represent a “late MI/MI–MII transitional” stage. In contrast, spindle-negative MI oocytes reflected an earlier phase of meiosis. This biological variability aligns with our clinical findings, in which MI oocytes contributed to embryo development and, in some cases, resulted in pregnancy. Spindle-positive MI oocytes may possess greater developmental competence due to more advanced nuclear organization, whereas spindle-negative oocytes likely have limited maturation progression. Thus, polarized light imaging may serve as a useful, non-invasive tool to discriminate the developmental potential of MI oocytes that fail to respond to rescue IVM, rather than discarding them uniformly. Overall, our findings indicate that a proportion of MI oocytes are not irreversibly immature and—with appropriate laboratory support—can yield clinically meaningful embryos. The pregnancy rate for MI oocytes was 25%, and live birth rate 12.5%, a promising result that highlights the potential of utilizing these oocytes in IVF treatments.
Another important consideration is fertility preservation through gamete vitrification. Ideally, vitrification should be performed on mature oocytes at the metaphase II (MII) stage, as this provides the best chance of future pregnancy. To maximize success, a large number of oocytes should be cryopreserved. Unfortunately, the time required for controlled ovarian hyperstimulation (COH) and oocyte retrieval often delays cancer treatment, leaving infertility specialists with limited opportunities to perform multiple cycles for cancer patients. As a result, freezing too few oocytes significantly reduces the likelihood of achieving a future pregnancy.In these cases, cryopreserving both MII and immature oocytes could be a viable option [15]. This study demonstrates that MI oocytes have the potential to result in pregnancy, supporting the notion that they should be frozen alongside their sibling MII oocytes.
There is also another perspective to consider. When a cancer patient has recovered and seeks pregnancy using her cryopreserved oocytes, IVF specialists thaw the oocytes. In situations where no mature oocytes survive the thawing process, MI oocytes can become a valuable resource. These oocytes can either be matured in vitro (IVM) and used once they reach full maturity or utilized as they are, as shown in this study. This highlights the importance of preserving MI oocytes as an additional option for fertility preservation.
As expected, MI oocytes exhibit compromised developmental competence. Mature oocytes play a critical role in achieving a successful pregnancy, and the use of immature oocytes is associated with poorer clinical outcomes in IVF/ICSI cycles. Even MII oocytes obtained after IVM show lower fertilization, blastulation, and pregnancy rates [16, 17, 18]. In vivo matured oocytes remain the optimal choice. For patients with a history of a low proportion of mature oocytes, several strategies can be employed to increase the number of in vivo matured oocytes. These include adding LH to COH protocols, using a double trigger with GnRH agonist and hCG, extending the interval between hCG administration and oocyte retrieval, modifying the IVF protocol, or changing the FSH type (recombinant or hMG). However, this topic is beyond the scope of this paper.
Rescue IVM has been described with different approaches in the literature, including both prolonged culture of immature oocytes and the direct use of MI oocytes after cumulus removal. In our study, the prolonged culture method was applied, which remains a subject of debate regarding its efficiency compared with direct MI injection. Nevertheless, our findings underline the critical role of assisted oocyte activation in supporting fertilization and embryo development from immature oocytes
The major strength of this study lies in its novel perspective on MI oocytes. Utilizing MI oocytes that do not respond to rescue IVM is an innovative approach in embryology clinics and may contribute to increased overall pregnancy rates. However, this study also has several limitations.
The first limitation is the small sample size, which restricts the generalizability of the findings. Further studies with larger sample sizes are necessary to validate these results.The second limitation is a selection bias in the study population. Only couples who did not have any embryos derived from in vivo or in vitro matured MII oocytes received an MI-derived embryo. This indicates that the investigated population had some degree of oocyte maturation defect or a low oocyte quality profile, limiting the universality of the findings. One other limitation is that none of the embryo transfers in this study were day 5 blastocyst transfers, and no preimplantation genetic diagnosis (PGD) was performed. As a result, this study cannot provide data on blastulation rates (the percentage of blastocysts obtained) or euploidy rates. These aspects should be addressed in future research. In addition, the developmental competence and safety of MI oocytes that fail to reach MII after short-term culture remain uncertain. The potential risk of transmitting aneuploidies or epigenetic alterations should be carefully considered before suggesting any clinical application. Therefore, the present study does not advocate immediate clinical use of such oocytes but rather highlights their potential and the need for further prospective research. Larger studies with structured designs, appropriate control groups, and detailed chromosomal and epigenetic analyses are warranted before clinical translation can be considered.
{kind=link}