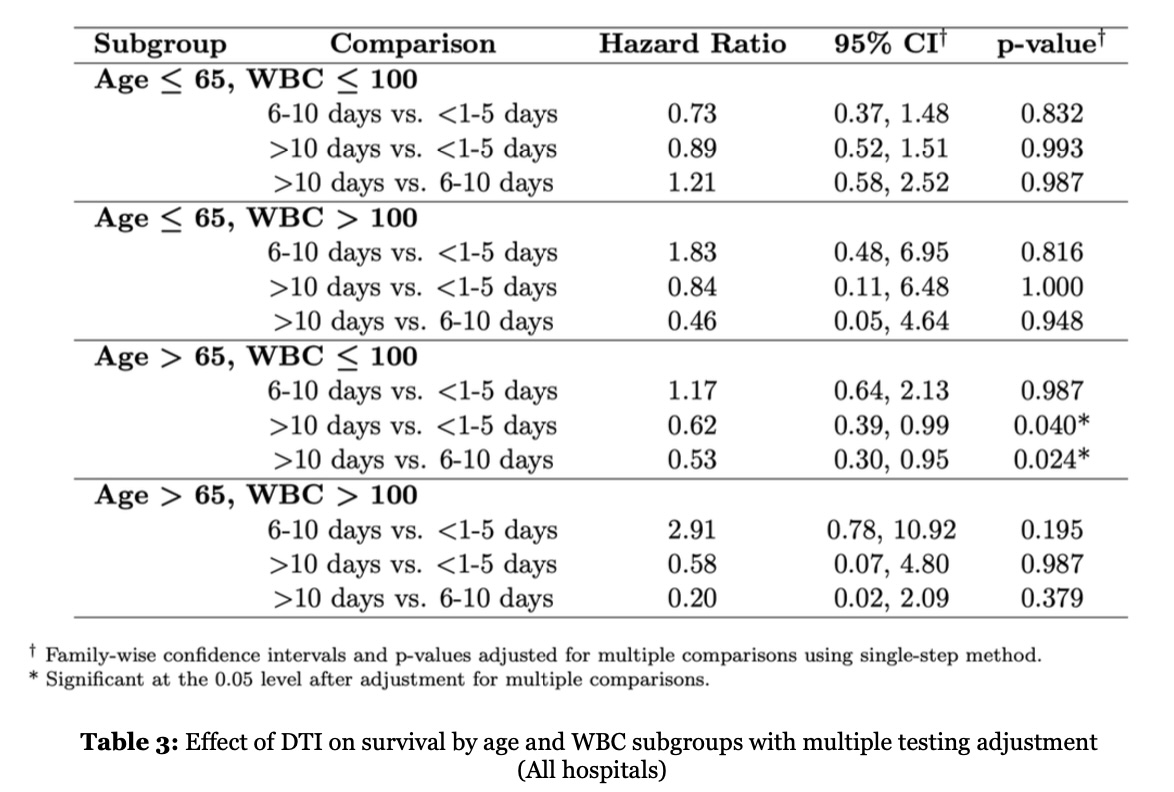
Our findings reveal an unexpected association between the DTI and outcomes in older patients with AML. Specifically, prolonged DTI was associated with reduced mortality in older patients, whereas no survival benefit was observed in younger patients. Even among young patients with elevated WBC counts, treatment delay did not significantly influence outcomes. This observation differentiates our analysis from prior large registry studies, such as the German Study Alliance Leukemia–Acute Myeloid Leukemia (SAL-AML) and TriNetX registry or reports by Röllig et al. and Bertolli et al, which found no significant impact of DTI on survival.11,12,13
Another large retrospective study of 1,317 patients from the Cleveland Clinic and the MD Anderson Cancer Center reported lower complete response (CR) and OS rates among young patients when DTI exceeded five days, while outcomes among older patients remained unaffected.6 Similarly, an ECOG study of 362 patients demonstrated lower CR rates with delayed therapy initiation, although this did not translate into an OS difference.13
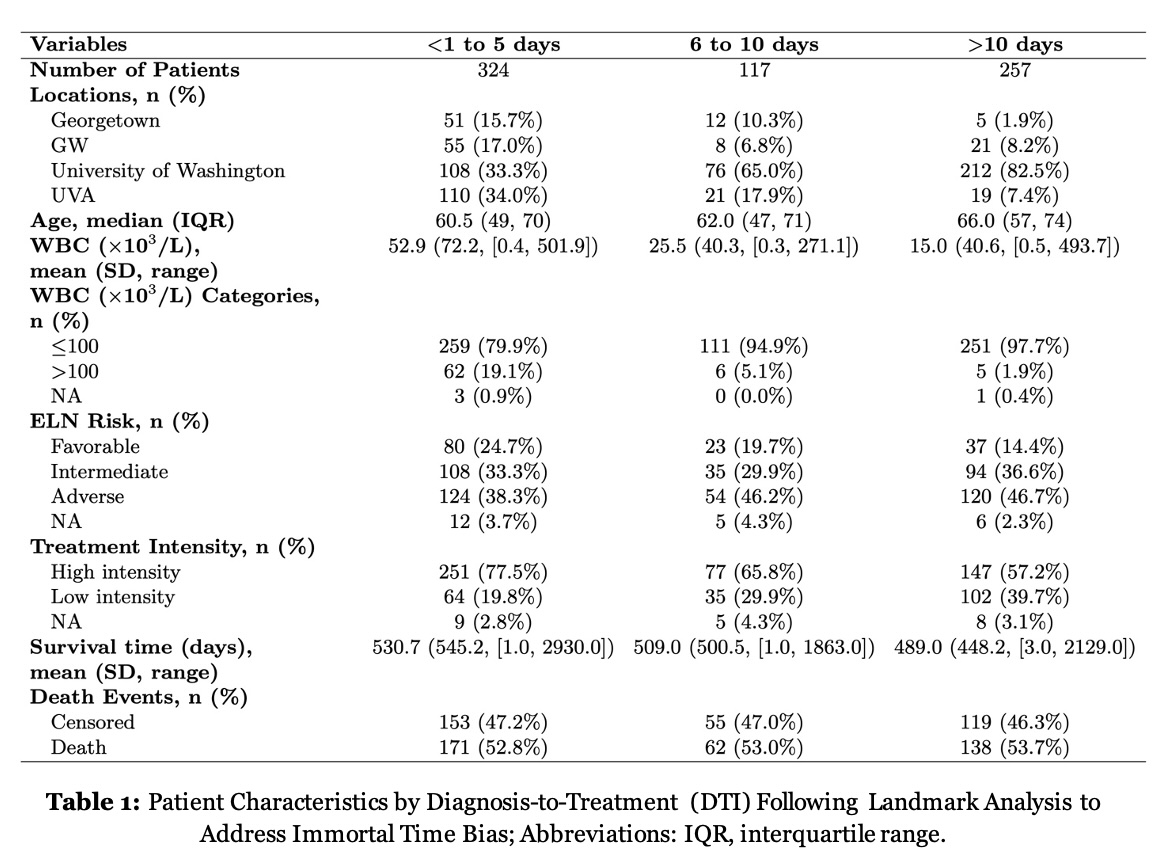
Evaluating the effect of DTI is inherently complex due to selection bias inherent to retrospective study designs. To mitigate this bias, we stratified patients by WBC count. Interestingly, even in patients with hyperleukocytosis, prolonged DTI did not adversely influence outcomes. Other potential confounders, such as disseminated intravascular coagulopathy (DIC), active infection/ or sepsis, and transfusion requirements, may also have contributed to differences in early mortality and treatment tolerance.
To our knowledge, this is the first study to demonstrate a potential adverse impact of shorter DTI in older patients with AML. Several explanations may account for this finding. AML is a biologically and clinically heterogeneous disease, and older patients who received therapy earlier may have presented with greater clinical instability or more aggressive disease features, prompting expedited treatment initiation. Such patients may also have been less physiologically fit, predisposing them to treatment-related complications and early mortality. Our dataset did not capture clinical parameters such as infection or DIC, which limits our ability to test this hypothesis directly. Furthermore, our cohort largely predated the widespread use of venetoclax-based regimens, which may limit applicability to contemporary treatment paradigms.14
Given these considerations, our results should be regarded as hypothesis-generating rather than definitive evidence of causality. Notably, prior studies examining DTI in AML have employed heterogeneous definitions of “delay”, with intervals varying widely across analyses. Some modeled DTI as a continuous variable, while others used categorical thresholds, as in our study. A prior meta-analysis suggested that median DTI across studies typically ranged from four to eight days.15
Our study has several limitations. First, its retrospective design introduces potential selection bias and confounding by indication, as patients perceived to be more acutely ill were likely prioritized for earlier treatment. Second, the landmark analysis, while essential to minimize immortal time bias, inherently excluded patients who died within 10 days of diagnosis, thereby limiting generalizability to early survivors. Third, data granularity was constrained: precise treatment initiation dates were unavailable, necessitating calculating of OS from the date of diagnosis rather than from the start of therapy. This approach, although standard, reflects the full disease trajectory rather than isolating post-treatment survival.
Conclusion In this multi-institutional retrospective study, a prolonged diagnosis-to-treatment interval was associated with improved survival among older patients with newly diagnosed AML, particularly those with lower white blood cell counts, while no adverse effect of treatment delay was observed in younger patients. These findings challenge the traditional assumption that immediate initiation of therapy universally improves outcomes and underscore the importance of individualized treatment timing in the era of precision oncology. Prospective studies are warranted to validate these results and to determine whether a brief delay to obtain comprehensive molecular data and optimize therapeutic selection may improve outcomes in clinically stable patients.
{kind=link}
{kind=link}
{kind=link}
{kind=link}