Hepatocellular carcinoma (HCC) is a common malignant tumor of the digestive system[1]. Despite various treatment methods, the prognosis for HCC remains generally poor. It has been confirmed that the anaerobic microenvironment is closely associated with the progression and poor prognosis of HCC. Hypoxia can promote apoptosis resistance, invasion, and metastasis of tumor cells, with hypoxia inducer (HIF-1α) serving as a key regulatory factor in hypoxia[2]. The hypoxia observed in HCC primarily arises from an imbalance between abnormal vascularization, leading to insufficient oxygen supply, and the high oxygen consumption of tumor cells. Elevated expression of the HIF-1α in tumor cells is strongly correlated with tumor proliferation, invasion, metastasis, and neovascularization[3, 4]. Furthermore, increased expression of HIF-1α can upregulate glucose transporters and their downstream proteins, enhancing the efflux of therapeutic drugs and inducing resistance to chemotherapy in tumor cells[5, 6]. Additionally, the oxygen deficiency in liver cancer leads to an imbalance in the REDOX state of tumor tissues and cells. In this regard, the association between abnormal liver cancer and glutathione (GSH) metabolism is highly significant[7]. GSH, serving as the main reducing ligand, is most abundant in the cytoplasm of tumor cells (2–10 mmol·L-1), far exceeding its extracellular concentration (2–20 µmol·L-1)[8, 9]. Moreover, the concentration of GSH in tumor tissues is approximately four times higher than that in normal tissues[10]. The high concentration of GSH in tumor cells forms a complex with metal chemotherapy drugs, reducing their entry into the cell nucleus and hindering DNA binding[11]. Additionally, GSH is more readily pumped out of the cell by multidrug-resistant proteins MRP1 and MRP2, significantly diminishing the effective concentration of intracellular cisplatin and enhancing drug resistance in HCC[12, 13]. The development of a tumor microenvironment (TME) caused by anaerobic glycolysis, characterized by a low extracellular pH and high cytoplasmic pH, is one of the main features of tumor tissue[14, 15]. This TME is an important factor inducing tumor occurrence, metastasis, and drug resistance[16]. In comparison to normal tissue, tumor tissue exhibits increased production of acidic products, intramembrane transport, and clearance barriers, resulting in the formation of an acidic extracellular microenvironment within tumors[14, 17]. Thus, targeting the TME of hypoxia, high GSH concentration, and the acidic microenvironment in tumor tissues and cells are crucial for HCC therapy[18–21].
Over the past year, the concept of "cuproptosis" and its related mechanisms have garnered significant attention. In 2022, Todd R. Golub and Peter Tsvetkov's team published an article titled "Copper induces cell death by targeting lipoylated tricarboxylic acid cycle (TCA) proteins" in Science[22]. This article introduced the concept of "cuproptosis," which quickly became a prominent research topic. The research team elucidated the mechanism behind "cuproptosis," a novel form of copper-dependent cell death that occurs through the direct binding of copper ions in mitochondrial respiration to the fatty acylated components of the TCA. This binding leads to the aggregation of fatty acylated proteins, down-regulation of iron-sulfur tuftin, activation of protein toxic stress, and ultimately, induction of tumor cell death. This study revealed that copper-dependent cell death is a distinct mode of cell death that differs from apoptosis. Even when the apoptosis pathway is blocked, copper ions can still induce cell death through an alternative pathway. Therefore, "cuproptosis" may prove effective against tumor cells that are resistant to apoptosis or DNA damage repair, such as chemotherapy-resistant cells[23, 24]. Thus, understanding the mechanism of "cuproptosis" can provide insights into a novel approach for HCC treatment. Furthermore, the mechanism of "cuproptosis" directly involves the tricarboxylic acid cycle in cellular mitochondrial respiration[25]. A high concentration of GSH, as a complex with copper ions, inhibits the occurrence of "cuproptosis"[26]. Consequently, the presence of high GSH levels and a hypoxic TME hinders the activation of "cuproptosis" in tumor cells. Therefore, investigating whether the effects of "cuproptosis" can be enhanced by providing peroxide oxygen supply to overcome the high concentration of GSH and hypoxic TME in tumors is of great significance. Currently, various copper ions and chelating agent carriers have been employed in preclinical and clinical tumor treatments[24]. Examples include the copper ionocarrier disulfiram (DSF) for glioblastoma, ATN-224 for breast cancer, and Elesclomol for melanoma, all of which are in Phase II clinical trials. However, the abnormal accumulation of copper in the body can harm an individual's overall health and well-being. Therefore, it is crucial to carefully administer copper ions within a specified therapeutic range. By utilizing a drug delivery system (DDS) to deliver more copper selectively to tumor cells, it is possible to achieve targeted tumor destruction while minimizing the toxic side effects of excess copper on the body[27]. In conclusion, the interaction between copper ions and peroxides in the tumor microenvironment presents an opportunity to overcome various adverse factors associated with "cuproptosis" activation in HCC. Through the clever design of a DDS based on peroxides and copper ions, a novel approach to liver cancer treatment can be explored.
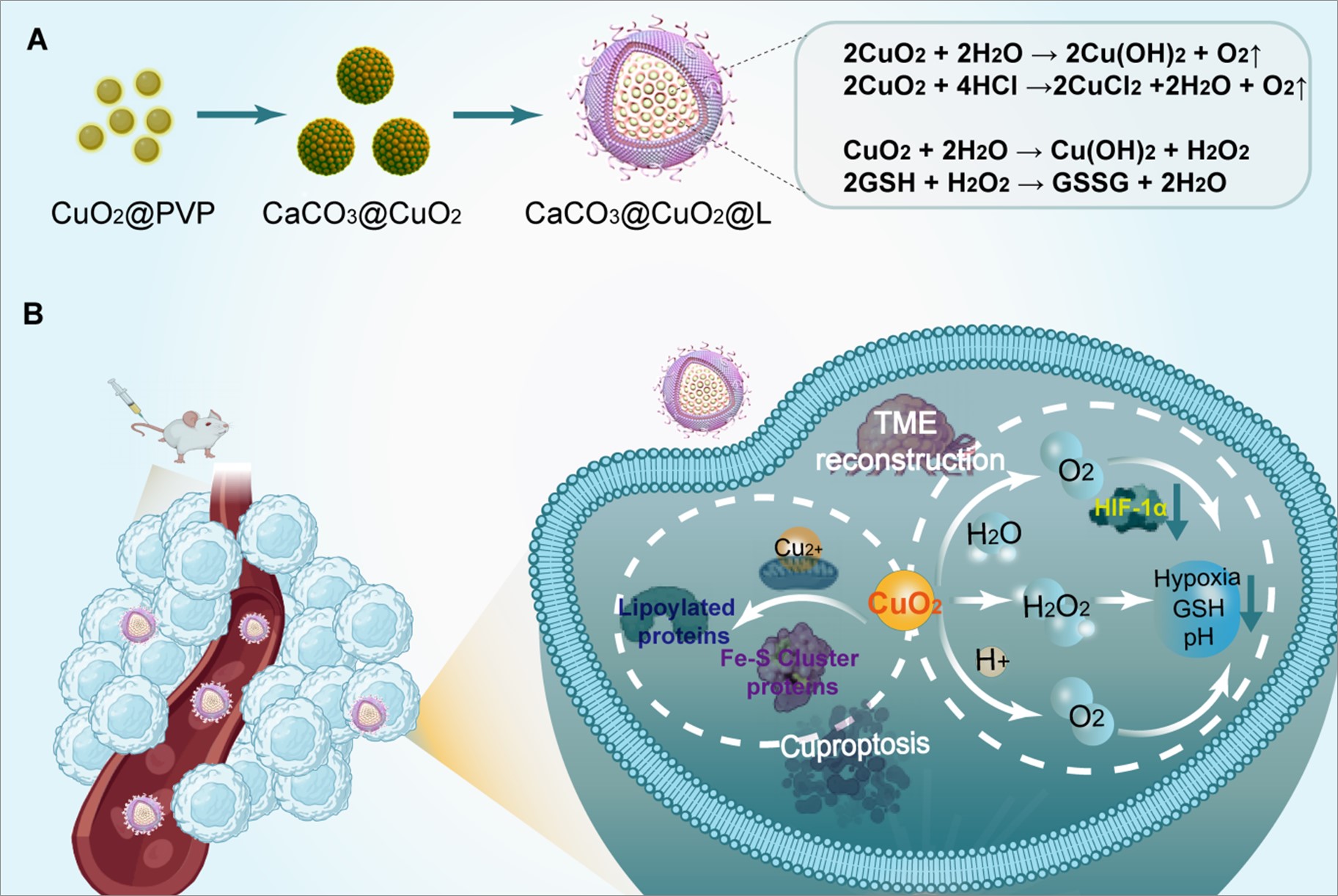
In our previous studies, we have reported various DDS targeting tumor hypoxia, utilizing peroxide nanoparticles[28, 29]. These systems have demonstrated effective regulation of tumor hypoxia, high concentrations of GSH, and acidic microenvironments. Building on this research, the current study aims to design and prepare a novel DDS using watermelon-type lipid-coated CaCO3@CuO2 nanoparticles (CaCO3@CuO2@L) through the reversed-phase microemulsion method. This preparation method is well-established, straightforward, and reliable. Over the years, we have utilized the reversed-phase microemulsion method to develop various DDS for investigating tumor hypoxia. Both in vivo and in vitro studies have demonstrated promising results. Firstly, the CaCO3@CuO2@L, prepared using the reversed-phase microemulsion method, exhibited uniformity and stability, with an average particle size of approximately 200 nm. Secondly, in vitro experiments revealed that CuO2 nanoparticles can decompose within the tumor acidic TME, generating O2, Cu2+, and OH−. Consequently, a continuous oxygen supply is generated, GSH levels are reduced, and pH is regulated. In HepG2 cell lines, the uptake of CaCO3@CuO2@L was effective. Furthermore, the nanoparticles successfully regulated hypoxia, reduced GSH levels, and increased pH in HepG2 cells. Additionally, CaCO3@CuO2@L effectively inhibited the growth of HepG2 cells, regulated oxygen deficiency, and activated pathways associated with "cuproptosis." Finally, the ability of CaCO3@CuO2@L to suppress liver cancer growth was demonstrated in vivo using orthotopic HCC and transplanted tumor models. In summary, this study builds upon the "trinity" concept of CaCO3@CuO2@L to comprehensively regulate the tumor microenvironment in HCC. By reconstructing the tumor microenvironment and inducing "cuproptosis", the growth of liver cancer is effectively inhibited, representing a promising approach for HCC treatment.
{kind=link}