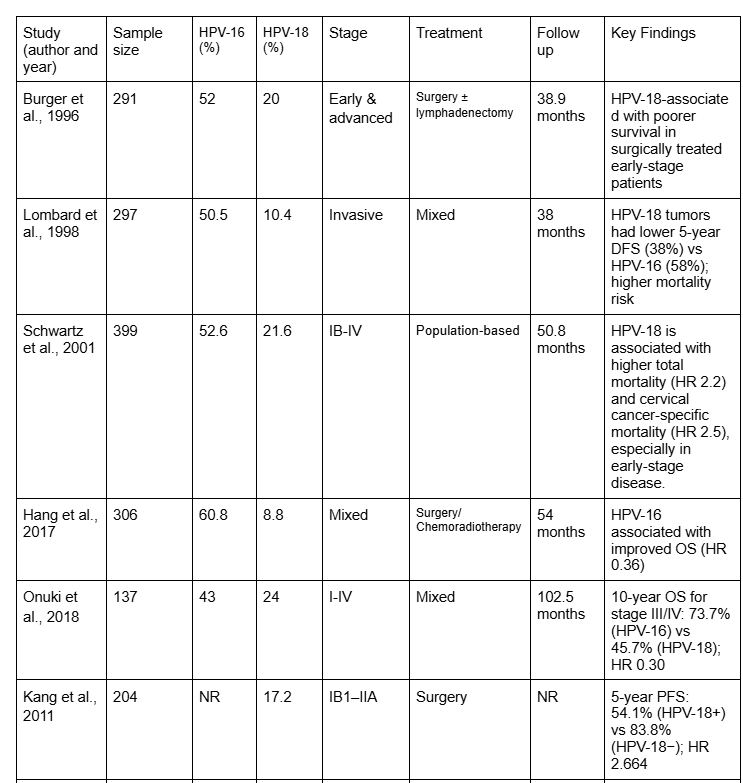
This systematic review brings together evidence from multiple cohort studies to examine how HPV-16 and HPV-18 affect prognosis in cervical cancer. Across nearly all included studies, HPV-16 was the most common genotype, accounting for approximately 40.5% to 69% of cervical cancer cases, while HPV-18 was less frequent, ranging from 8.8% to 33.3% (Hang et al., 2017; Mata et al., 2021). Despite its lower prevalence, HPV-18 consistently demonstrated a stronger association with poor clinical outcomes. In contrast, HPV-16 positivity was generally linked to improved overall survival (OS) and disease-free survival (DFS), particularly in patients with advanced-stage disease (Onuki et al., 2018; Hang et al., 2017).
Several studies reported that patients with HPV-18-positive tumors experienced higher recurrence rates and increased mortality, especially in early-stage cervical cancer. This pattern highlights an important biological and clinical distinction between HPV-16 and HPV-18, even though both are considered high-risk genotypes (Schwartz et al., 2001; Lombard et al., 1998; Kang et al., 2011). These findings suggest that HPV genotype plays a meaningful role in determining patient outcomes and should not be viewed as interchangeable across disease stages.
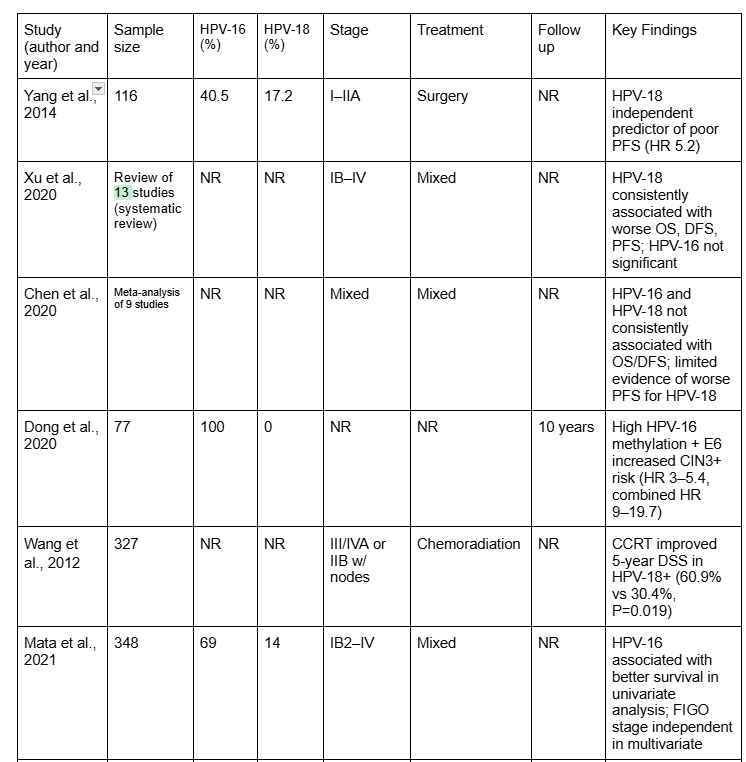
In advanced-stage cervical cancer (FIGO stages III–IV), HPV-16-positive tumors were associated with significantly higher overall survival compared to HPV-16-negative tumors (Onuki et al., 2018). This observation suggests that HPV-16-positive tumors may respond more effectively to chemoradiotherapy. On the other hand, HPV-18-positive tumors showed higher hazard ratios for disease progression and death, particularly in early-stage disease (Burger et al., 1996; Yang et al., 2014). These trends align with the findings from the meta-analyses, which reported that HPV-18 consistently predicts worse progression-free survival (PFS) and DFS, while HPV-16 shows limited prognostic impact in early-stage disease (Xu et al., 2020; Chen et al., 2020).
The observed differences in prognosis between HPV-16 and HPV-18 may be explained by underlying biological mechanisms. HPV-16 is most commonly associated with squamous cell carcinoma, which tends to be detected earlier and respond more favorably to treatment. In contrast, HPV-18 is more frequently linked to adenocarcinoma, a subtype often associated with aggressive tumor behavior and poorer outcomes (Burger et al., 1996; Lombard et al., 1998).
Variations in the expression of viral oncogenes, particularly E6 and E7, may further influence tumor growth, treatment response, and survival. Dong et al. (2020) demonstrated that epigenetic changes in HPV-16, such as DNA methylation combined with E6 oncoprotein expression, can help stratify long-term risk for high-grade cervical lesions (CIN3+). These findings highlight the complex interaction between HPV genotype, viral gene regulation, and cancer progression.
HPV genotype may also play an important role in determining response to treatment. Wang et al. (2012) reported that patients with HPV-18-positive advanced-stage squamous cell carcinoma experienced significant survival benefits from concurrent chemoradiation therapy (CCRT), whereas HPV-16-positive patients did not show the same level of benefit. This suggests that HPV-18-positive tumors may be particularly sensitive to combined treatment approaches.
In early-stage disease, HPV-18-positive tumors were associated with higher recurrence rates following surgical treatment, emphasizing the need for closer monitoring and consideration of adjuvant therapy in this patient group (Yang et al., 2014; Kang et al., 2011). Overall, these findings support the integration of HPV genotyping into clinical decision-making, not only for screening but also for prognostic evaluation and treatment planning.
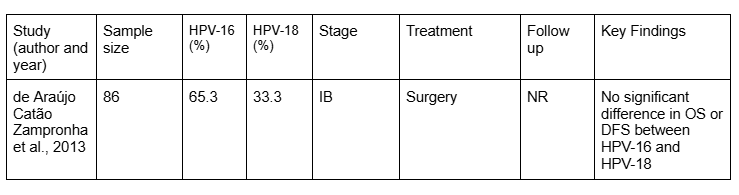
In contrast to advanced-stage disease, several studies found that HPV genotype had limited prognostic value in early-stage cervical cancer treated surgically. De Araújo Catão Zampronha et al. (2013) reported no significant differences in OS or DFS between HPV-16- and HPV-18-positive tumors, with both groups demonstrating five-year survival rates exceeding 90%. Similarly, Mata et al. (2021) found that while HPV-16-positive and α-9 species tumors appeared to have better outcomes in univariate analysis, FIGO stage was the only independent predictor of survival in multivariate analysis.
These findings suggest that when early-stage cervical cancer is completely resected, tumor stage may be a stronger determinant of prognosis than HPV genotype alone.
The results of this review are consistent with prior studies identifying HPV-18 as a negative prognostic factor (Xu et al., 2020; Chen et al., 2020). Historical cohort studies have also reported reduced OS and DFS among HPV-18-positive patients (Lombard et al., 1998; Schwartz et al., 2001). This review highlights stage-specific differences, showing that HPV-18 has a particularly negative impact in early-stage disease, while HPV-16 appears to confer a survival advantage in advanced-stage tumors (Onuki et al., 2018).
Several limitations should be considered when interpreting these findings. To begin, heterogeneity across studies in terms of their design, sample size, follow-up duration, and treatment strategies may affect their comparability. Furthermore, differences in HPV detection methods, such as PCR, DNA hybridization, or DNA chip assays, could influence genotype classifications. Third, most included studies were observational, limiting the ability to establish causation. Finally, this review primarily focused on HPV-16 and HPV-18, while other high-risk genotypes were not consistently evaluated, which represents an important gap in literature. Data extraction and study selection were conducted by a single reviewer, which may increase the risk of bias.
Future research should prioritize prospective, multi-center studies with standardized HPV testing methods, detailed reports of tumor characteristics, and long-term follow-up. Incorporating molecular and epigenetic markers, such as DNA methylation patterns and viral oncoprotein expression, may further refine risk stratification and improve personalized treatment strategies (Dong et al., 2020). Clinical trials examining genotype-specific responses to chemoradiation and emerging therapies are especially needed for HPV-18-positive patients, who consistently demonstrate higher-risk profiles.
{kind=link}
{kind=link}
{kind=link}