Colorectal cancer (CRC) is one of the most common and deadly types of cancer in the world. In 2022, nearly two million people were diagnosed with CRC, and over 900,000 died from the disease globally (World Cancer Research Fund, 2025; World Health Organization, 2023). It is the third most common cancer and the second leading cause of cancer-related deaths, making it a significant concern (World Cancer Research Fund, 2025). CRC primarily affects adults over the age of 50, but in recent years, the number of cases in adults under the age of 50 has been rising, a phenomenon called early-onset colorectal cancer (Roshandel et al., 2024). This suggests that the factors aren’t simply related to age but are possibly related to lifestyle, genetics, and environmental influences.
Several factors contribute to the risk of developing CRC. Genetic predispositions, such as Lynch syndrome or familial adenomatous polyposis, and a personal or family history of colorectal cancer, may increase risk (World Health Organization, 2023; Roshandel et al., 2024). Modifiable risk factors include lifestyle choices, such as a diet high in processed or red meats, low intake of fruits and vegetables, physical inactivity, obesity, smoking, and heavy alcohol consumption (World Health Organization, 2023). Additionally, psychological stress and changes in gut microbiota have been suggested as potential contributors to CRC risk, although more research is needed to fully understand these relationships (Roshandel et al., 2024). People with inflammatory bowel diseases, such as Crohn’s disease or ulcerative colitis, and those with prior abdominopelvic radiation exposure are also at higher risk (Roshandel et al., 2024).
Prevention and early detection are key strategies in reducing CRC incidence and mortality. Primary prevention includes adopting a healthy diet, maintaining regular physical activity, avoiding tobacco and excessive alcohol, and managing body weight (World Health Organization, 2023). Secondary prevention involves screening for CRC using stool-based tests such as fecal occult blood tests (FOBT) or fecal immunochemical tests (FIT), colonoscopy, sigmoidoscopy, or stool DNA tests (Roshandel et al., 2024; World Health Organization, 2023). Early detection through these methods allows for the removal of precancerous polyps or early-stage tumors, which significantly improves survival rates. Screening guidelines differ slightly between organizations, as the American Cancer Society recommends starting at the age of 45, while other organizations suggest beginning at the age of 50 (Roshandel et al., 2024).
Despite advancements in prevention, screening, and treatment, CRC remains challenging to manage, especially in stage II and III cases. Surgery is the main curative treatment that is often combined with chemotherapy or radiation therapy, depending on tumor stage and risk factors (Fan et al., 2024). However, even after curative-intent surgery, 20–30% of patients experience cancer recurrence, meaning that cancer cells remain undetected in the body (Negro et al., 2025). Doctors traditionally rely on clinical and pathological markers, such as tumor stage, lymph node involvement, tumor grade, and blood markers like carcinoembryonic antigen (CEA), to predict which patients are most at risk of recurrence (Fan et al., 2024). While these markers provide some guidance, they are not always accurate. Additionally, some patients may receive more chemotherapy than necessary, which results in side effects. On the other hand, others may not receive enough, which can lead to residual cancer being untreated (Negro et al., 2025).
In response to these challenges, researchers have developed and tested circulating tumor DNA (ctDNA) as a new tool for monitoring CRC. ctDNA consists of DNA shed by tumor cells into the bloodstream, carrying tumor-specific mutations (Chidharla et al., 2023; Fan et al., 2024). Because ctDNA has a short half-life, usually only a few hours, it allows for real-time monitoring of cancer in the body. The detection of ctDNA is minimally invasive compared to traditional tissue biopsies and provides an understanding of the patient’s cancer status. Studies have shown that patients who test positive for ctDNA after surgery are far more likely to experience recurrence, even if they undergo chemotherapy. On the other hand, ctDNA-negative patients generally have better outcomes (Negro et al., 2025).
ctDNA also has the potential to guide treatment decisions. For example, stage II and III patients who are ctDNA-positive may benefit from adjuvant chemotherapy, while ctDNA-negative patients could potentially avoid unnecessary treatment (Fan et al., 2024). This approach allows for more personalized therapy, which reduces the risk of harmful side effects from overtreatment while focusing resources on patients who truly need it. Moreover, ctDNA can detect minimal residual disease (MRD) earlier than traditional imaging or blood tests, sometimes months before a tumor would become visible on scans (Chidharla et al., 2023). Additionally, monitoring and tracking ctDNA over time has been shown to provide insight into disease progression, relapse, and response to therapy
Research Gap
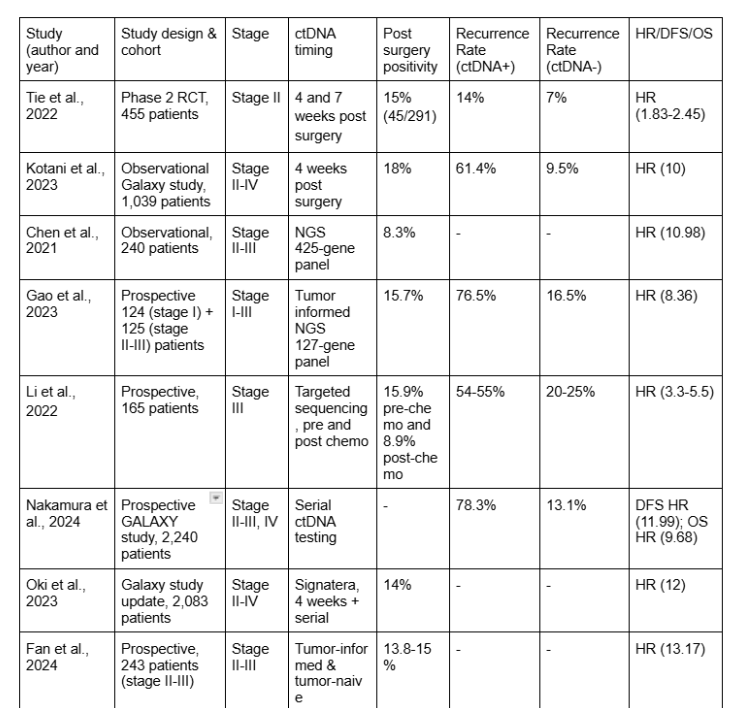
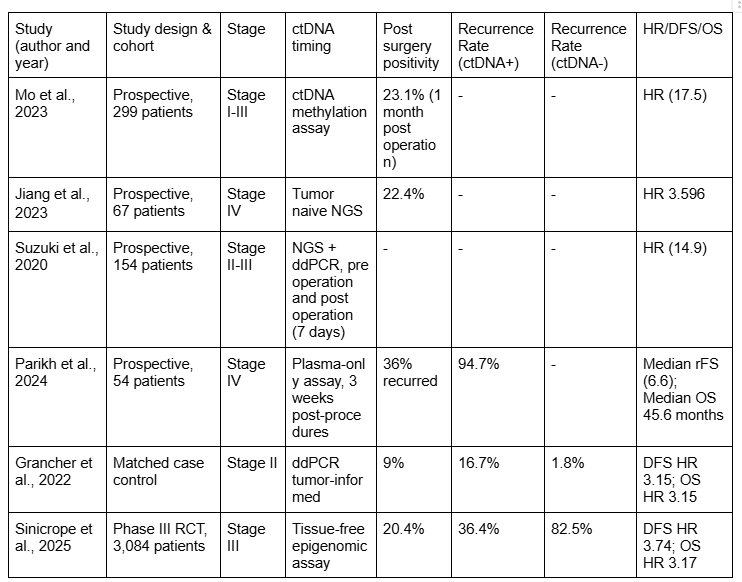
Although ctDNA shows an enormous amount of potential, there are several limitations and unanswered questions. Different studies use varying detection methods and thresholds, measure ctDNA at different time points, and define positivity differently, which makes direct comparison challenging (Chidharla et al., 2023; Negro et al., 2025). Many studies are also small, single-center trials, which may not represent the broader population. There is also limited understanding of how ctDNA adds value beyond traditional markers such as tumor stage, lymph node involvement, microsatellite instability (MSI) status, or CEA levels (Fan et al., 2024).
Longitudinal ctDNA monitoring has highlighted patterns of recurrence risk, such as patients converting from negative to positive or clearing ctDNA after chemotherapy, but this has not yet been analyzed systematically across multiple studies (Negro et al., 2025). Another important limitation is the sensitivity of ctDNA detection at certain metastatic sites, including liver-only or peritoneal metastasis, which can sometimes produce false negatives (Fan et al., 2024). Furthermore, there is also no consensus on the best timing or frequency for ctDNA testing, nor on the standardization of assays, which limits its clinical implementation (Chidharla et al., 2023). These findings were consistent across multiple cohorts, supporting the robustness of longitudinal ctDNA dynamics as a prognostic marker rather than a study-specific effect.
Because of these gaps, an analysis combining multiple studies is needed. A systematic review and narrative meta-analysis could examine the prognostic power of ctDNA in stage II and III CRC, evaluate its value alongside traditional markers, standardize definitions, and clarify how serial testing can improve treatment decisions long-term (Negro et al., 2025; Fan et al., 2024). Addressing these gaps would not only improve patient care but could also reduce the need for unnecessary chemotherapy exposure, minimize side effects, and provide earlier interventions for patients at high risk of recurrence.
Overall, colorectal cancer is a major global health issue with increasing incidence and high mortality. Traditional risk markers for recurrence are helpful but not perfect, leaving a need for a more precise tool. ctDNA has the potential to be a promising biomarker that can detect minimal residual disease, predict recurrence, and guide therapy decisions. However, limitations in standardization, timing, and comprehensive evaluations create a research gap. Conducting systematic studies and meta-analyses will be essential for determining how ctDNA can be integrated into routine clinical practices, ultimately improving survival and quality of life for CRC patients (Chidharla et al., 2023; Negro et al., 2025; Fan et al., 2024).
Study Objectives
The primary purpose of this systematic review and narrative meta-analysis is to evaluate how well postoperative circulating tumor DNA (ctDNA) can predict recurrence in patients with stage II-III colorectal cancer who have undergone surgery.
The study will assess how ctDNA positivity after surgery is linked to recurrence, disease-free survival (DFS), and overall survival (OS). It will also compare how well ctDNA predicts outcomes compared to traditional markers, such as tumor stage, nodal status, and CEA levels. It will examine how changes in ctDNA over time, such as persistent positivity, clearance, or conversion from negative to positive, affect patient outcomes. It will evaluate whether using ctDNA to guide chemotherapy can better target treatment and avoid unnecessary therapy for low-risk patients. Finally, it will assess if combining ctDNA with other risk factors, such as tumor characteristics or molecular markers, improves predictions of recurrence.
Overall, this study aims to provide clear evidence on how ctDNA can help doctors personalize treatment, detect recurrence early, and improve care for stage II-III colorectal cancer patients.
{kind=link}
{kind=link}