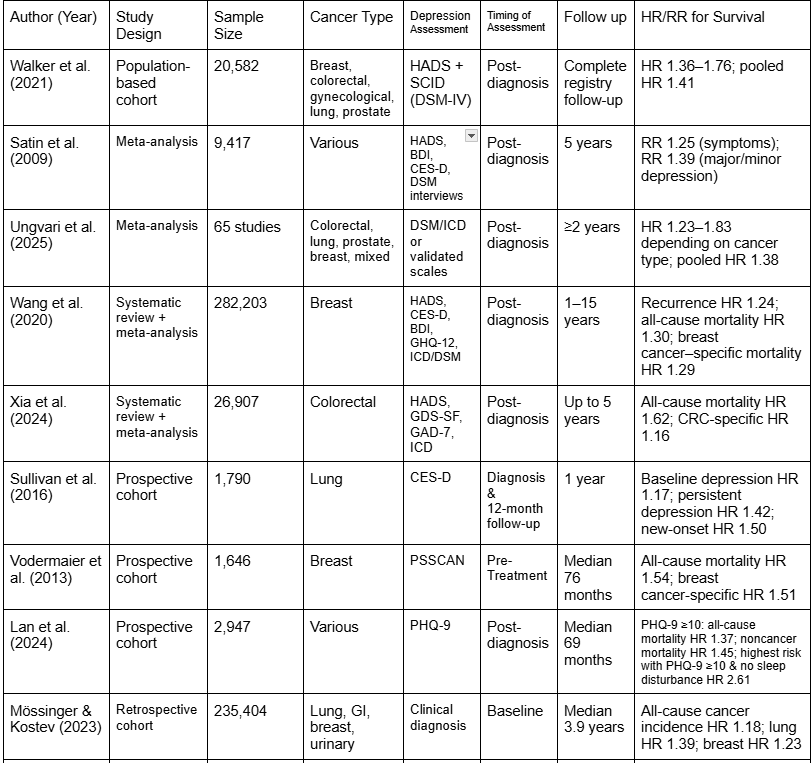
Across the 12 included studies, depression was assessed using either validated symptom-based instruments or a structured clinical diagnostic criteria. Clinically diagnosed depression was typically defined using DSM or ICD criteria derived from psychiatric interviews or medical records (Satin et al., 2009; Walker et al., 2021; Yen et al., 2022). Symptom-based assessments most commonly used the Hospital Anxiety and Depression Scale (HADS), Center for Epidemiologic Studies Depression Scale (CES-D), and Patient Health Questionnaire (PHQ) instruments (Vodermaier et al., 2013; Sullivan et al., 2016; Lan et al., 2024).
Follow-up duration ranged from approximately 3 years to over 15 years across cohorts. Most studies adjusted survival analyses for key clinical covariates, including age, cancer stage, treatment modality, and comorbidity burden, allowing evaluation of depression as an independent prognostic factor (Pinquart & Duberstein, 2010; Walker et al., 2021; Xia et al., 2024).
Across nearly all the included studies, depression was associated with significantly worse overall survival (OS) among patients with cancer. Early meta-analytic evidence by Satin et al. (2009), which included 25 studies with clinically diagnosed depression and 26 studies using symptom scales, demonstrated that depression was associated with a significantly increased risk of mortality. The pooled effect size was strongest for studies using clinical diagnoses, with hazard ratios approaching 1.39, while symptom-based measures showed smaller but still significant effects.
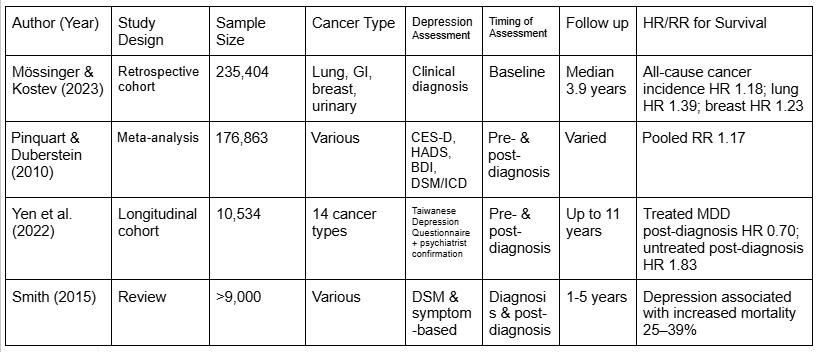
Pinquart and Duberstein (2010) further expanded upon this evidence in a meta-analysis of 76 prospective studies, reporting a pooled relative risk of 1.17 for cancer mortality among depressed patients. Importantly, this association remained significant after controlling for demographic variables, disease stage, and treatment factors in the majority of included cohorts, supporting depression as an independent prognostic factor rather than a simple correlation of disease severity.
More recent large-scale cohort studies reinforced these findings. Walker et al. (2021) analyzed over 20,000 cancer patients using a two-stage psychiatric diagnostic process and found that major depression was independently associated with increased all-cause mortality across multiple cancer types (adjusted HR 1.41). The association persisted when analyses were restricted to cancer-specific mortality, suggesting that the observed effect was not driven solely by non-cancer causes of death.
The prognostic impact of depression varied based on timing and severity. Several studies demonstrated that depression diagnosed after cancer diagnosis had a stronger association with mortality than pre-existing depression (Satin et al., 2009; Walker et al., 2021). This suggests that depression emerging in response to cancer diagnosis or treatment may reflect biological or behavioral processes more directly relevant to disease progression.
Severity and persistence of depressive symptoms further modified risk. Sullivan et al. (2016), in a longitudinal study of lung cancer patients, identified distinct depression trajectories and showed that patients with persistent or worsening depressive symptoms experienced significantly higher mortality compared to patients with transient or remitting depression. In contrast, patients whose depressive symptoms resolved over time had survival outcomes comparable to those of non-depressed patients.
Similarly, Lan et al. (2024) reported that moderate-to-severe depressive symptoms were associated with markedly increased long-term mortality among cancer survivors, whereas mild symptoms showed weaker and less consistent associations.
Evidence for the prognostic role of depression was consistent across several cancer types. In breast cancer cohorts, depression at diagnosis or during early treatment was associated with worse OS and increased recurrence risk (Vodermaier et al., 2013; Wang et al., 2020). Wang et al. (2020), in a meta-analysis of over 280,000 breast cancer patients, reported that depression significantly increased the risk of both mortality and disease recurrence, with the strongest effects observed in patients with comorbid anxiety.
In lung cancer, depression demonstrated particularly strong prognostic significance. Sullivan et al. (2016) reported that persistent depression was associated with significantly higher mortality independent of disease stage and treatment. These findings are consistent with earlier observations that psychological distress may be especially impactful in cancers with aggressive disease courses.
In colorectal cancer, Xia et al. (2024) analyzed a large population-based cohort and found that depression independently predicted all-cause mortality after adjustment for tumor stage, treatment, and comorbidities. Although associations with cancer-specific mortality were weaker, the overall survival disadvantage remained significant.
Several studies provided evidence that depression is a potentially modifiable prognostic factor. Yen et al. (2022) examined over 19,000 cancer patients with diagnosed depression and demonstrated that adherence to antidepressant treatment or psychiatric care was associated with significantly improved survival compared to untreated depressed patients. Notably, untreated depression was associated with the highest mortality risk, exceeding that observed in non-depressed patients.
Similarly, Sullivan et al. (2016) observed that remission of depressive symptoms over time mitigated excess mortality risk, suggesting that effective treatment may reverse some of the adverse prognostic effects associated with depression.
{kind=link}
{kind=link}