Short-term clinical efficacy of VAS-based programming. The advent of multi-segmented electrodes has greatly increased DBS programming complexity due to numerous parameter combinations. Recent advances in aDBS for PD use electrophysiological biomarkers like local field potentials (LFPs) for dynamic parameter adjustment,42 yet structured integration of patient-reported feedback remains lacking in electrophysiology- or image-based approaches for ET and other conditions. Here, we evaluated the short-term clinical efficacy of VAS-based programming in ET. Consistent with previous findings,26 no significant differences were observed between VAS-based and standard programming (Fig. 1a,b), supporting subjective patient feedback as a valid DBS programming signal. Notably, VAS-based settings achieved similar outcomes with lower stimulation amplitudes (Fig. 1c), suggesting reduced energy use and battery drain without loss of efficacy—an important factor given that battery replacements are a leading cause of DBS-related infections.43 These results underscore the need to reconsider high-amplitude reliance and to integrate patient experience into DBS parameter adjustments (Fig. 1e).
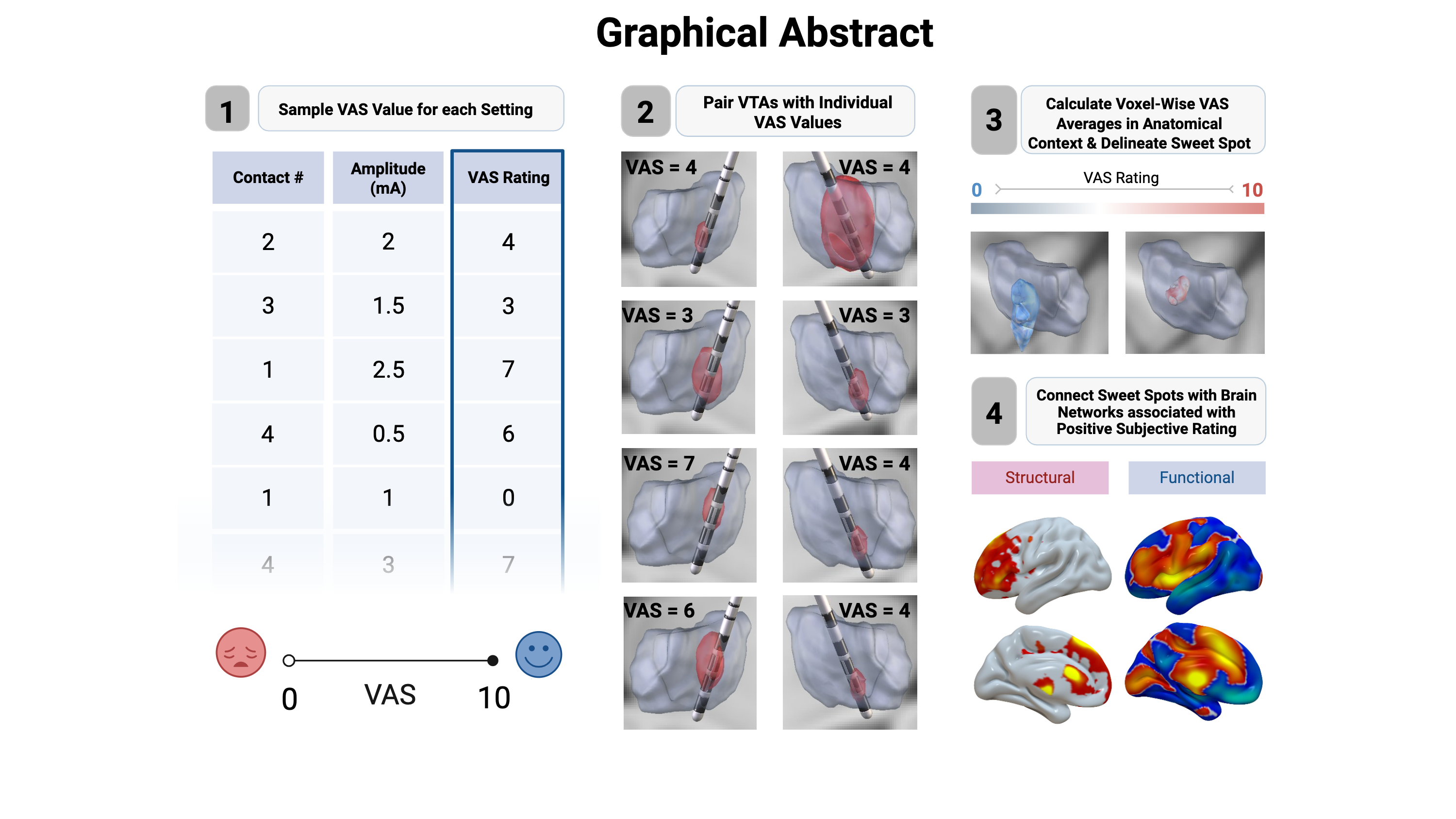
Subjective sweet and sour spots: Treatment success inET-DBS is largely determined by choosing the most effective target structure. Whereas the VIM has traditionally been regarded as an effective target for tremor control,44 more recent results suggest stimulation sites caudal to the VIM to be most effective.13,20,45–47 Some studies imply that the proximity of the VTA to the DRTT was associated with greater tremor suppression efficiency15,16 and that the distance to the DRTT is more critical for clinical efficacy than specific coordinates,17–19,48 suggesting that different target regions may represent a common anatomical fibre tract – the DRTT.21,49 In accord, the PSA, including the cZi, Forel field H, and the prelemniscal radiation, was proposed as an effective and alternative stimulation target for ET. In fact, several studies proposed that PSA-DBS might have better efficacy in controlling tremor symptoms and cause fewer stimulation related side effects.15,50–54 Other studies have also postulated the existence of stimulation sweet spot more anteriorly in the region of the ventralis oralis posteriornucleus (VOp) or along the VIM/VOp border.46,55,56 By pairing VAS scores with VTAs, we identified regions with the highest and lowest subjective ratings—termed the “subjective sweet” and “sour” spots. The sweet spot localized dorsally within the VIM, while the sour spot lay posteroventrally, below the VIM (Fig. 2b). This contrasts with reports placing the tremor sweet spot more ventrally, possibly due to side effects or negative subjective sensations not evident in clinical exams. The VAS sweet spot was near the DRTT, whereas the sour spot was farther from its ventral entry into the VIM, consistent with effective tremor control involving DRTT engagement (Fig. 2d).Overall, our findings emphasize incorporating patient feedback when selecting ventral contacts in VIM-DBS and support the concept of outcome-specific sweet spots, as recently described in PD.57 Future prospective studies should compare these distinct sweet spots in terms of clinical efficacy and patient satisfaction in chronic ET-DBS.
Connectivity of subjective sweet spots in ET: Recent DTI-based connectivity studies on thalamic DBS suggest that the cerebello-thalamo-cortical network plays a key role in tremor modulation 58. Strong connectivity between active DBS contacts and network nodes is assumed to be linked to therapeutic effects. Some studies focused on specific network nodes 59, while others analysed whole-brain connectivity using patient-specific or normative connectome data 20,45. For instance, Akram et al. used probabilistic tractography to show high structural connectivity between the VIM and M1, SMA, S1, and contralateral dentate nucleus 45. Grimm et al. examined 20 ET patients who had undergone bilateral DBS using patient-specific probabilistic diffusion tensor imaging, identifying that the connectivity of the M1, and somatosensory cortex, was most closely related to complete and incomplete tremor suppression, with the anterior lobe of the cerebellum and SMA also involved 60. Similarly, Al-Fatly et al. identified the patterns of effective VIM-DBS connectivity by normative brain connectomes, found that there was positive connectivity in multiple regions, mainly in the paracentral gyrus, visual cortex, and superior and inferior cerebellar lobules 13,20. Our study investigated the structural and functional connectivity associated with the VTA and its correlation with subjective patient feedback. We identified significant positive structural connectivity between the subjective sweet spot and brain regions including the prefrontal and frontal lobe, and the insular cortex (Fig. 4). On the one hand, our sweet spot is indeed located close to the DRTT aligning closely with these above-mentioned studies58,61. However, our results also suggest additional connectivity patterns. The involvement of the frontal and prefrontal regions, as well as the insular cortex, in our connectivity analysis is particularly noteworthy. The prefrontal and superior frontal cortices are central to executive control, decision-making, and cognitive flexibility, while the inferior frontal gyrus is implicated in inhibitory control and motor planning.62,63 Notably, the prefrontal cortex has also been implicated in affective responses to DBS.64 The insula, in turn, serves as a hub integrating interoceptive awareness, affective processing, and salience detection.65 Taken together, these regions contribute to the cognitive and emotional dimensions of symptom perception. In the context of our results, connectivity of the subjective sweet spot to these cortical areas may reflect the integration of motor improvement with higher-order evaluative and affective processes that shape patients’ VAS ratings. This suggests that subjective feedback during DBS titration may not solely depend on sensorimotor tremor suppression but also on cognitive and affective appraisal mediated by prefrontal and insular circuits.
LIMITATIONS
This study has several limitations. First, data were collected in an acute setting, capturing only short-term effects; thus, long-term outcomes of VAS-based programming remain unknown. However, as tremor typically responds to DBS within seconds,10 our conclusions likely extend to longer periods. Future studies should include long-term follow-up to confirm this. Second, self-reported measures may be influenced by mood or cognitive bias; combining subjective ratings with objective clinical and biomarker data would yield a more comprehensive assessment. Third, the small, single-center sample limits generalizability and may explain the low statistical significance of the identified sweet spot. Larger, multicenter studies with diverse populations are needed to validate these findings and allow subgroup analyses across DBS targets or conditions.
{kind=link}